
Hormone Replacement Therapy
- May 16
- 23 min read
Hormone Replacement Therapy (HRT, for short) is a transitional method many trans guys undertake to alleviate gender dysphoria. Typically, HRT is comprised of taking synthetic testosterone (colloquially known as "T" or "test") in injections or a topical gel. There are many effects that happen to the body when taking synthetic testosterone, though medical research about T is still in its infancy.
There is no one or "correct" way to take T. The dosage and application method are entirely up to the individual and their care provider. Below is information consolidated from medical professionals and real trans guys on their experiences taking testosterone.
No one at the Trans Guy Archive is a medical professional and nothing on this page should be interpreted as explicit medical advice. If you have serious medical questions, contact your doctor or care provider.
(click to jump)


















A Short History of HRT

Hormone Replacement Therapy (HRT, for short) has not been widely available for most of human history. Only during the 20th century were scientists and doctors able to synthesize the hormones to create artificial (but still effective) hormone replacements. Initially, drugs such as Premarin were made from pregnant horse urine, though Premarin is typically prescribed to cisgender women experiencing menopausal symptoms. Many forms of synthetic hormones are derived from natural origins, though many are are entirely lab-created.
With testosterone in particular, the first recorded instance of it being synthesized was in 1935 by Adolf Butenandt in Germany. Previously, synthetic masculinization had been observed in experiments where animal testes were transplanted onto other animals. While he may have not been the very first, Dr. Michael Dillon was among early candidates for masculinizing HRT, obtaining a prescription in 1939. Dr. Dillon is also notable for being the first ever recorded trans man to undergo gender confirmation surgery (aka "bottom surgery").
Currently, synthetic testosterone is more widely available. Many high-performing athletes and movie stars take forms of synthetic testosterone (which typically have a host of names: "test", "gear", "roids", etc.). For the average trans guy, testosterone is available via prescription from a doctor/endocrinologist.
Effects of masculinizing HRT
Do you have photos of yourself experiencing these changes? We would love to upload them here to show people what to look for!
The Physical
Your skin will become thicker and more oily as your pores largen and oil production increases.
The smell of your sweat and urine may change. Typically your sweat becomes 'muskier' smelling. Some trans guys report a chlorine-like body odor at times.
Fat deposits in certain parts of your body will begin to redistribute. Typically, fat in your thighs and butt will shift toward your abdomen (stomach). This can help you look less curvy, though your bone structure will not change, with some rare exceptions.
Your breasts may shrink a little and become a bit saggy. This is due to the lower amount of estrogen in the area.
Gaining muscle will become easier! With the right diet and exercise, many trans guys taking testosterone find their legs and arms have more muscle definition, often with more prominent veins and a slightly rougher appearance.
Your eyes and face may begin to change shape as fat redistributes. Many trans guys taking testosterone experience "tom cat-ification" where their cheeks become very round for a while as their body adapts to the initial changes.
Your vocal chords will begin to thicken and your voice will begin to drop, akin to how cisgender boys' voices drop during puberty. Your voice early on testosterone may sound squeaky or similar to a vocal fry (colloquially known as "T-voice"), but voice training can slowly fix this. Issues of vocal fry may resolve itself on its own after taking testosterone for many years. Your voice will begin to drop within a few weeks of starting testosterone and will not reach full maturity for at least 5 years.
Body hair will become more prominent. Hair on your chest, back, and arms will increase in thickness and will become darker. It will also grow at a quicker rate than before. You MAY develop male pattern baldness if other cisgender men in your family also have the condition. Unfortunately, male pattern baldness is not curable, but can be treated with topical medications such as finasteride, minoxidil, etc. Even if you do not experience male pattern baldness, hair thinning on the front of your scalp is relatively common.
You may begin growing facial hair. This result varies heavily from person to person and each person's facial hair will have different degrees of thickness and coverage. Starting testosterone later in life (40 and above) may result in less overall facial hair growth than those who start at younger ages. Using hair growth treatments like minoxidil may promote the growth of facial hair, though be warned that minoxidil is extremely toxic to household pets!
There may be vaginal dryness and partial atrophy of the vaginal walls. Not everyone experiences dryness to the same degree. It can be temporarily treated with a water-based lubricant, or treated long-term with a topical estrogen cream - don't worry, the cream isn't strong enough to 'undo' the effects of testosterone.
Eventually, you may see menstruation slow and/or totally cease. If you experience spotting/bleeding randomly after not experiencing it for a while, talk to your doctor. Some trans guys taking testosterone may not experience a cessation of menses at all. Ironically, an excess of testosterone may return your periods, so it is important to keep to your prescribed dosage.
After a short time, your clitoris will begin to lengthen and widen. It will also increase in sensitivity. Many people experience uncomfortable chafing against their underwear as the clitoris grows (often referred to as "bottom growth"). Most trans guys taking testosterone will average 1 to 2 inches of erection after growth slows. The size of your growing clitoris depends on genetics. Some 'pump' their clitorises in an effort to increase their size, though it is not confirmed that will make a long-term difference.
The Mental
You will begin to experience emotions differently. Many trans guys taking testosterone report increased anger, depression, and anxiety. Thankfully, these are all manageable symptoms. Taking testosterone will NOT make you permanently angry, depressed, etc. Many report these feelings lessening the longer they've been on HRT and with external help (e.g. medication/therapy).
Your libido will skyrocket, especially for those on higher doses. You will frequently become aroused, even by small things. You may find that different things arouse you than prior to starting testosterone. Your kinks and tastes in people may also change. Many trans guys taking testosterone report feeling a stronger romantic/sexual attraction to men/masculinity.
Orgasms will feel different. Rather than a pleasant, whole-body rush, the orgasm may feel entirely consolidated in your clitoris, lending to the feeling of being "shot" with pleasure.
Your appetite will increase. You may often feel ravenous, or that you're hungrier more frequently than you were prior to taking the medication. There is not a specific reasoning why this is, though take caution with overeating.
Potential Risks
No medication comes without potential risks. Weigh the risks with your doctor or care provider before starting testosterone. Take note that these are POTENTIAL risks. There is a chance you will not experience any of these, but it doesn't hurt to stay alert.
Testosterone HRT is not birth control. It may lessen your ability to become pregnant, but as long as you have your uterus and ovaries (and were not completely sterile to begin with), there is a chance of conceiving if you have sex with a person capable of producing sperm.
If you are looking to conceive a child, your doctor will instruct you to stop taking testosterone, as the medication is fatal to the fetus. You are still able to take birth control, including non-hormonal kinds. You are also still able to take "day-after" types of birth control like Plan-B (though as an external precaution, medications like Plan-B have a weight limit).
It is unclear if testosterone HRT contributes to an increased risk of high cholesterol and heart disease. Unfortunately, long-term studies are lacking. If you and/or your family has a risk of these conditions, talk to your doctor about ways to mitigate risks.
Testosterone may make your blood thicker, otherwise known as a high hematocrit count. This can potentially lead to a stroke, heart attack, or other conditions relating to the heart. If you and/or your family has a risk of these conditions, talk to your doctor about ways to mitigate risks.
It does not appear that testosterone HRT increases the risk of cancer to the uterus, ovaries, or breasts. However, data is still limited and caution should still be considered. During top surgery, they do not remove 100% of the breast tissue, so there is still a theoretical risk of breast cancer.
While you do not have a prostate (to the extent someone AMAB does), there is emerging research surrounding a sort of "pseudo-prostate" that trans guys begin to grow while on testosterone HRT. It is currently unclear if trans guys who have been on HRT for an extended time have to screen for prostate cancer.
If you have had one or both of your ovaries removed, it is critical to remain on at least a low dosage of hormones until approx. the age of 50. This will help your bones to remain strong and avoid early onset osteoporosis.
Some migraines and autoimmune conditions can improve or worsen. The science behind this is currently unclear. Talk to your doctor or care provider with any overlapping concerns.
SOME EFFECTS OF TESTOSTERONE ARE IRREVERSIBLE. These are: hair loss on your scalp, voice deepening, facial and body hair growth, and clitoral enlargement. Otherwise, every other effect is reversible (though results may vary).
YOU CANNOT PICK AND CHOOSE WHAT EFFECTS YOU GET. As annoying as this may be, taking testosterone is similar to a regular genetic lottery. For example, if you don't like having facial hair you can shave/laser it off, but it won't stop growing.
MICRO-DOSING TESTOSTERONE WILL NOT PREVENT SPECIFIC EFFECTS FROM HAPPENING. Micro-dosing HRT is not "I'm only going to get X number of effects". It is more like "I'm going to get 100% of my intended effects, but at a slower rate than a standard dose". For example, if you are genetically predisposed to male pattern baldness, micro-dosing testosterone will not 100% prevent baldness, but it will slow the rate at which it inevitably happens to you.
Anecdotal Effects
While there are side effects from testosterone that are clinically proven, some trans guys report anecdotal effects from the medication -- which means these effects have not been professionally studied and come from the patient's own personal experiences. Like all the other side effects listed above, these may or may not affect you.
If you recognize a risk that may affect you in this section, talk to your doctor.
One person reported that their fibroadenoma (benign breast tumors) went away after taking T. They reported giant painful lumps that shrank over time and completely went away after their testosterone treatment.
One user on Tumblr reported that switching from injections to gel caused their period to come back.
Using a copper-based IUD (Intrauterine Device) led to one internet user getting painful cramps and inconsistent cycles, despite being 1.5 years on testosterone. His doctor was unsure how a hormone-based IUD would effect his transition.
More frequent vaginal infections stemming from testosterone-induced vaginal dryness. It doesn't necessarily mean you will feel literally "dry" but can still be a discomfort.
Vaginal dryness can be treated with a topical estrogen ointment. This can be prescribed by your doctor. In an emergency/short-term situation (eg, sexual intercourse), use a water-based lubricant.
Testosterone may help ease pain and discomfort brought on by endometriosis. Testosterone is not known to make endometriosis worse.
One trans man on TikTok reported that his Raynaud's Disease significantly diminished after taking testosterone for multiple years.
One trans man on Instagram reported that he has had significantly fewer epileptic seizures after taking testosterone for multiple years.
Testosterone can be rarely used to treat adenomyosis.
Reports of hair becoming curlier and/or oilier and/or thinner
Timeline of masculinizing effects
Below is a table showing the expected onset of mental and physical effects from taking testosterone HRT. Remember, these are expected timelines. Some people see changes early, others see them much later. This is a general guide to when you should expect to see changes. You also may not experience every change on this list.

What dosage is right for me?
There is no "one dosage fits all" criteria. Those wishing for a more binary transition may have a higher + more frequent dosing schedule than those who only wish to change things subtly. You can typically choose between injectable testosterone or have it in a topical gel form. Dosing is entirely up to you and what you wish to get out of HRT.
Consult the chart below regarding what "level" of dosing you may prefer when speaking to your doctor. They may recommend a different/lower dose to start you out on.

Which is better? Shots (injections) or Gel?
Generally speaking, T is T, and the application you choose does not make a HUGE difference in how your body processes the medication. The dosage of the medication makes more of a difference than the application, but this section covers the various methods of taking testosterone HRT, as well as the risks and benefits of each.
Gel sometimes comes in the form of a patch or topical cream.

Easy clean up.
Only needs to be done once a week, every other week, or at a less frequent schedule (dependent on the dosage).
No risk of spreading medication side effects/toxicity to pets and (human) loved ones.
Cost effective (one 1mL vial can last up to a month, depending on dosage).
Injections can be done in a timely manner.
Slower withdrawals if multiple doses are skipped.
There are auto-injectors for people who want shots but are afraid of needles. These are less likely to be covered by insurance though (at least in America).

Injecting a needle can be painful.
You must have a continual supply of needles, alcohol wipes, and (optional) bandages on hand.
May prove difficult to travel with on airplanes/across country borders.
Injections have a carrier oil - cottonseed, grapeseed, olive, sesame, etc. Some individuals may be allergic to one or more of these oils.
Injections can cause mild soreness in the area where the needle entered the body, typically for 1-3 days post-injection.

Easy application (topically applied to the skin).
Good for those with needle phobias.
More consistent hormone levels (if applied daily, regularly).
Easy to travel with (can be stored in travel-size containers).

Generally more expensive than injections.
You have to let the medication dry on your skin before touching anyone or anything with that area of your body. You also cannot swim or engage in physical activity that would get your skin sweaty.
Not letting the gel dry fully can risk it rubbing off on other people/pets. T-Gel is toxic to animals. The medication rubbing off on another person, consistently over time, can lead to them getting dosed with your medication. While that may seem beneficial if this other person is a fellow trans guy, it really means that (A) you aren't getting the correct dosage, and (B) the other trans guy may be getting too much testosterone, which can lead to adverse effects.
Have to apply it every single day, or as instructed by your care provider.
Can potentially cause dry skin/eczema in the area the medication is applied to.
Quicker noticeable withdrawals if multiple doses are skipped.
How to access testosterone HRT
Accessing hormones through a clinic is a process that typically takes multiple months. You will...
Get a referral to see an endocrinologist. They specialize in treating the endocrine system, which covers hormone replacement therapy. If possible, find an endocrinologist that already has experience treating trans people in your age group. Depending on how busy the doctor is/if they're accepting new patients, this may take several months.
Have a consultation with your endocrinologist. They will ask you about your health history, including if your family has a history of heart problems, high cholesterol, high blood pressure, and/or mental illness. When possible, answer them honestly, especially if there is a history of high blood pressure/cholesterol/heart problems. The doctor will likely, at some point, also give you an Informed Consent sheet to read and sign, along with other paperwork to indicate you understand the side effects and potential risks of taking testosterone.
Below is an example of an Informed Consent sheet to look over and provide to your endocrinologist in the event they haven't heard of it before.
Your endocrinologist will need to do some bloodwork to clear you for hormone replacement therapy. A typical blood panel will test for:
Free Testosterone/Testosterone/Testosterone BIOAV
Estradiol
LH (Luteinizing Hormones)
Lipid panel - Cholesterol, Triglycerides, HDL/LDL cholesterol, CHOL/HDL CHOL ratio, non-HDL cholesterol
CBC + Platelets
Hemoglobin
Your endocrinologist may also have you schedule several appointments to speak with a psychiatrist (at Mt. Sinai in New York City they typically have you schedule 3 appointments, one per week) prior to your first injection/application of testosterone.
Usually after that you're cleared to start HRT! Congrats on getting this far!
How to apply T-Gel
First, locate an optimal spot on your body for applying your gel. This spot must be:
over muscle
not especially bendy (like your joints)
not at risk of accidentally rubbing off on other people/pets
not covered by clothing
Typical spots for applying T-Gel are:
The upper arms and shoulders, avoiding the armpits and inside of the elbows.

The front and backs of your thighs, avoiding behind the knee joint and your groin.

The abdomen. Some studies have suggested T-Gel doesn't get absorbed as well through this area, but data is still inconclusive.
Then, wash your hands with warm water and soap. Use the pump of the bottle or open the gel packet and squeeze the contents onto your skin in your selected area.
Rub the gel in a circular motion into your skin. Allow several minutes for the gel to dry completely before you put clothes over the area. Drying time depends on the brand of T-Gel, your environment, and any skin conditions you may have.
Congrats on applying T-Gel!
Important:
NEVER apply T-Gel to your genitals. It will BURN and it will HURT. Applying T-Gel to your genitals will NOT make your clitoris grow faster or bigger. You will need a DHT (compound testosterone cream) for that.
How to administer injections
Subcutaneous (SubQ)

Subcutaneous (SubQ) injections are delivered into the subcutaneous muscle (seen in diagram at right) beneath the skin. SubQ injections have a more gradual, steady absorption rate into the body, as well as a slower onset of side effects. They also require minimal training with some medical instruction.
The needle used for SubQ injections is thinner and shorter than a needle used for Intramuscular (IM) injections. SubQ injections are usually administered with 23 to 25 G (gauge), 5/8" (inch) needles.
They are typically done into the ABDOMEN, THIGH, or BACK OF THE ARM.
YOU WILL NEED:
23 - 25G, 5/8ths of an inch syringes - can be purchased on sites like Amazon or gotten via your insurance provider
testosterone medication (typically comes in 1mL vials)
Alcohol wipes/pads
Band-Aids (or favorite brand of bandage)
TO-DO:
Gather all your materials. Sanitize the work area with a disinfectant wipe, if available.
Wash hands well with soap and warm water.

Remove syringes from plastic packaging. Draw the plunger back so the FLAT TOP of the black rubber stopper lines up with your correct dosage.
Uncap the testosterone vial. Wipe the rubber seal with an alcohol wipe/pad.

Uncap the syringe, making a rainbow motion with your hands to avoid accidental poking. Hold the vial in one hand, the syringe in the other. Insert the needle into the vial -- keeping the tip of the needle fully submerged into the medication -- and flip the vial upside down, holding it between your index and middle finger (similar to a peace sign). Use your ring and pinky finger to hold the syringe stable. If another hand position is more comfortable, use that.

Pull the plunger back. The medication is in a thick oil, so it will take up to 30 seconds to draw up the full dose. Using a syringe with a SMALLER gauge (which means a larger opening) will speed up the process. Once you have drawn up the correct dose, remove the needle from the vial and recap the needle carefully.
If you draw up more medication than needed, push the plunger back up until you have reached approximately your desired dosage. NOTE: you will likely lose a little medication when transferring needle tips; so to avoid this, draw up a little more than you need.
Before moving on to the next step, if you are transferring needle tips, pull the plunger all the way back so the medication is sucked out of the needle tip and you maintain the correct dosage.
If you are using two needles, open the other syringe from its package. In a swift motion, unscrew the capped needle of syringe 1 (the one you just drew the medication up with) and swap it out for the capped needle of syringe 2 (which will be sharper than the needle of syringe 1; this will make the injection hurt less).
Gently push the plunger back up so the top of the black rubber stopper lines up with your correct dose. Hold the needle up to a bright light and watch for a faint gleam or shimmer of the medication at the tip of the needle as you push the plunger up -- this is to remove all pockets of air in the needle.
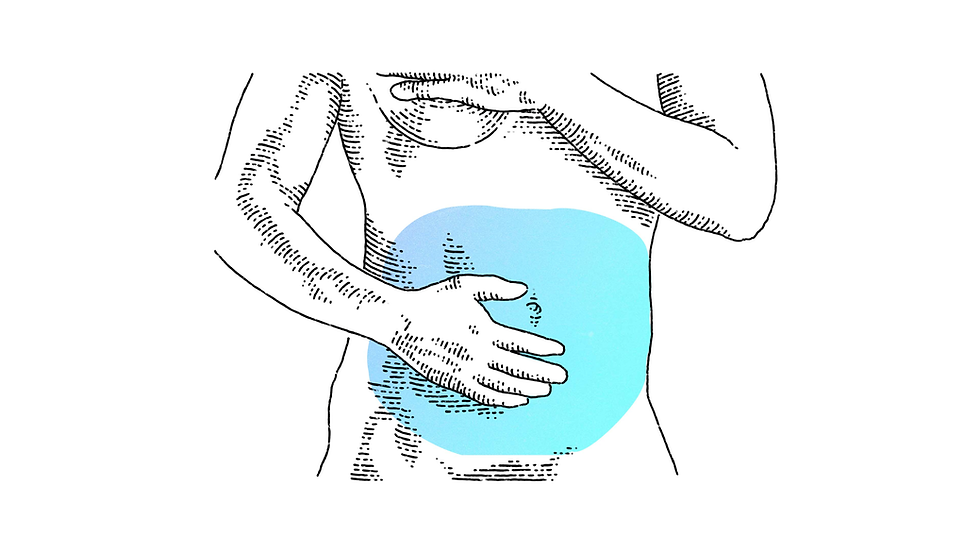
Identify the area you will be injecting the medicine. Typical areas are highlighted in blue below.

image courtesy of Memorial Sloan Kettering Cancer Center. With the alcohol pad, wipe down the intended injection zone. Carefully uncap the needle in a rainbow motion (like an upside down-U).
Hold the needle as if holding a dart or pen. Gently pinch the skin where you intend to inject. Then, insert the needle QUICKLY at a 45 degree angle. Going slowly will hurt a LOT.
Push the plunger down to inject all the medicine. Once the plunger has been pushed down all the way, leave the needle inside your body for about 5-10 seconds to prevent leakage. Then, pull the needle out in one swift motion at the same 45 degree angle you injected at.
Carefully re-cap the needle and apply a bandage to the injection site, if needed.
Clean everything up and carefully dispose of needles in a sharps-box.
Congrats on your first injection!






Still unsure how to administer a SubQ injection? Check out these videos below!
Intramuscular (IM)

Intramuscular (IM) injections are delivered into the muscle (seen in diagram at right) beneath the skin. IM injections have a quicker absorption rate into the body, as well as a quicker onset of side effects. They also require a good amount of training with some medical instruction.
The needle used for IM injections is thicker and longer than a needle used for Subcutaneous (SubQ) injections. There will be more needle entering your body. IM injections are usually administered with 23 - 25 G (gauge), 1" or 1.5" (inch) needles.
They are typically done into the THIGH, SHOULDER, or (the muscle above your) BUTTOCKS.
If you choose to inject into your thigh, you will not inject directly into the top or directly into the side -- aim for a 3/4ths angle. Measure the distance by putting a finger on one hand at your hip and another finger on your other hand at your knee, then draw them together to find the middle. Do this lengthwise and widthwise on your thigh to find the approximate 3/4ths angle.
Consult the chart below for the optimal injection site.

YOU WILL NEED:
23 - 25G, 1 inch OR 1.5 inch syringes - can be purchased on sites like Amazon or gotten via your insurance provider
testosterone medication (typically comes in 1mL vials)
Alcohol wipes/pads
Band-Aids (or favorite brand of bandage)
Note from Aidrian: I personally give myself Intramuscular injections; not for any personal reason, that was just what my clinic trained me to do. If you're administering these shots to yourself, the thigh is the easiest place, though the buttock is objectively the sexiest.
TO-DO:
Follow the step-by-step instructions in the Subcutaneous injection section (above) up until Step 10. After that, follow the steps listed here.
Hold the needle as if holding a dart or pen. Take two fingers and 'flatten' (NOT PINCH) your skin around the injection site. This is to prevent skin bunching and to make sure the needle makes it to the muscle below the skin and fat.
Holding the needle at at 90 degree angle, quickly inject yourself in one motion. If you are using a 1-inch needle: the entire needle should enter your body. If you are using a 1.5-inch needle: you only need to get about 3/4ths of the needle in your body.
Push the plunger down to inject all of the medication.
After the plunger has been pushed down the entire way and no medication is left in the syringe, hold the needle inside your body for 5-10 seconds. This is to prevent medication leakage.
Remove the needle at a 90 degree angle, in one swift motion.
Carefully re-cap the needle and apply a bandage to the injection site, if needed.
Clean everything up and carefully dispose of needles in a sharps-box.
Congrats on your first injection!
Still unsure how to administer an IM injection? Check out these videos below!
Gallery of testosterone HRT changes
Some photos found publicly on the internet showcasing the different changes while taking testosterone.


















If you would like to add/remove your photo, please let us know!
Testosterone HRT FAQ
Want to add a question you were wondering about? Contact us!
How frequently should I be injecting T?
Injections schedules can vary person to person. For the most consistent hormone levels, it is recommended to inject yourself once, weekly. You can also inject every two weeks (aka every other week), though this may lead to you hitting a deeper trough* right before your next injection.
*trough = the lowest point in your hormone cycle. The side effects of testosterone will be noticeably few or absent during this time.
How often should I be applying my T-gel?
Every day, or as instructed by your doctor. You can choose what time of day to take it, depending on your school/work schedule.
How long should I wait to let my T-gel dry?
About 10 to 60 minutes, depending on the brand.
What is considered a "normal level" for my testosterone to be at?
Under 18 yrs of age: approx. 100-970 ng/dl
18 and over: approx. 300-1080 ng/dl
Important Note: if your testosterone level falls anywhere within the appropriate range, then you are fine. Even if you're "scoring low". Higher levels of testosterone do not necessarily mean you will be stronger, manlier, etc. In fact, the higher your testosterone levels, the higher likelihood of your body converting it back into estrogen.
Note from Aidrian: My T levels have been pretty consistently around 400 and I look like a lumberjack, so don't fret too much about the numbers on the chart.
Is testosterone legally available without a prescription?
Short answer: No.
Longer answer: Testosterone is considered a "controlled substance" by the FDA (and by similar govt. orgs around the world), which means that it is heavily regulated. Legally, all vials/bottles of testosterone require a prescription to be written by your doctor/care provider and then approved by your insurance (if applicable), who will sometimes need to complete a "prior authorization" to confirm whether or not you still "need" the medication. This process may take a week or more, so plan your dosing accordingly!
The TGA may add more information about DIY HRT at a later date, but for now do your best to go through legal channels, where available. It's the best method for keeping yourself safe with a doctor's help.
Can I take testosterone pills?
NO! DO NOT TAKE PILLS! One of the lesser talked about side effects of testosterone is the wear on the liver, which filters the chemicals found in your blood. Testosterone pills (which are typically sold by sketchy "health" companies that prey on the patriarchal insecurities of cisgender men) will cause serious damage to your liver and will NOT give you the desired side effects that you're looking for.
What about testosterone pellets?
Yes! Testosterone pellets -- different from pills -- which are placed underneath the skin, are safe to take. They are typically implanted near the buttocks and will slowly and steadily release testosterone for 2-6 months, though they are commonly replaced around month 3. This does require mild surgical intervention and may or may not be covered by your health insurance. Talk to your doctor if you're interested in testosterone pellets.
What size and gauge of needle should I get for injections?
For most people who take SubQ or IM injections, you will need two (2) needles - one to draw the medication up from the vial, and another to inject it into your body. Needle sizes are backward from typical counting, which is to say the bigger the number, the smaller the needle hole. For reference, an epidural needle is approximately 16-18G (gauge).
For drawing up your medication, we recommend needles that are 18-20G and 1-inch in length. For injecting, we recommend needles that are 23-25G and EITHER 5/8-inch, 1-inch, or 1.5-inch long, depending if you are performing a SubQ or IM injection.
Do I need to get my syringes through my insurance?
Not necessarily. While it is cost-effective, some insurances won't cover the type of needles you need. You can buy a bulk box of syringes at online stores like Amazon or at local medical supply warehouses for cheap. Be sure to get the correct length and gauge! Aim for luer-lock syringes.
Is it normal for a little bit of my injected testosterone to leak out of the hole?
Yes. The inside of the human body is highly pressurized, so any hole introduced into the muscle/skin will allow medication to escape. A little dribble is totally normal. Anything more than that you may have to speak with your doctor about.
When doing injections, one way to prevent leakage is, after you've fully pressed the plunger of the needle down, hold the needle inside your leg for about 5-10 seconds, then pull the needle out in a swift motion. This will allow the medication to begin its journey into your body and not spring back up through the injection site immediately.
What is the difference between testosterone cypionate and enanthate?
Testosterone cypionate (aka Depo-Testosterone):
Longer half-life (usually 7-8 days), fewer injections required
Carrier oils tend to be cottonseed, grapeseed, olive, etc. (thinner, easier for injecting)
Typically less expensive than enanthate
More common in the USA
Testosterone enanthate
Shorter half-life (usually 4-7 days), more suitable for smaller, quicker doses
Carrier oil is usually sesame (some people may be allergic + it is more viscous, which can be more uncomfortable to inject)
Typically more expensive than cypionate
More commonly found in Europe/internationally (outside the USA)
All in all, there is actually very little difference between the two, outside of their carrier oils. Go with whatever your doctor prescribes.
Is it normal for the injection site to get itchy and swollen after a shot?
No. Mild soreness in the area is expected, but if you are experiencing any of the above symptoms or pain in the area, you may be allergic to something in the medication. Consult your doctor immediately and contact Poison Control if the severity is high.
How often should I go in to get my bloodwork checked?
For the first year, you should be getting bloodwork done about every 3 months.
After the first year (and assuming there aren't any underlying issues), you can lessen your visits to every 6 months.*
*Or as directed by your care provider.
If I inject/apply more testosterone than my prescribed dosage, will my transition go faster?
No. In fact, excess testosterone can actually stall your transition, because it gets converted by your body back into estrogen.
Will testosterone make me infertile?
Assuming you are not totally infertile to begin with -- no. HRT is not birth control. If you sleep with someone who is capable of producing sperm and no barriers* were used, there is a possibility of becoming pregnant.
If you are looking to become pregnant or preserve your eggs for future pregnancy, consult your doctor before starting testosterone. If you wish to become pregnant, you will not be able to continue taking testosterone, as it is fatal to the growing fetus. You will also likely be put on estrogen medication to put your body into a state that is fertile enough for a baby to grow. You will be able to resume testosterone after the pregnancy/egg collection.
*barriers, such as condoms, dental dams, birth control, etc.
I started T a little over 8 months ago and I don't look like Hercules yet. Is it all over for me?
Not at all! Though you may see changes at a more rapid pace during your first year, you won't reach "maturity" for at least 5 years, if not more.
Remember -- you're going through a second puberty. You're starting back out like a 13 year old cisgender boy, so you're going to get everything they get -- the ratstache, a squeaky voice, random boners, etc -- and you'll "complete" puberty at about the same pace they would as well. It typically takes about 10 years to complete puberty. Your life will keep going on anyway.
Someone on Tumblr said testosterone is poison and will make me a monster.
This is (unfortunately) a classic example of TERF (trans exclusionary radical feminism) rhetoric. Testosterone and estrogen are simply biological hormones -- "evil" is an entirely human-made concept. Likewise, a person is not evil by having an excess/absence of a specific hormone. While testosterone can make you moodier and more irritable, these are not traits that are set in stone.
Don't fall for the hateful idea that men and masculinity are inherently evil. Masculinity is beautiful and powerful; and it is not a "corrupting" force.
I've heard going on T makes you more susceptible to heart disease and stroke.
Not necessarily. If there is no history of high cholesterol, high blood pressure, and/or stroke in your family history, then you have little to worry about. If this is a concern for you, talk to your doctor about ways to mitigate risks.
Does bottom growth hurt super bad?
Not necessarily. You will likely experience soreness in and around your clitoris as it grows, but it is not painful in the way a bruise or wound are. Trans guys on the thinner side (in regards to weight) may experience chafing and rubbing of the clitoris against their underwear, which can increase sensation. Trans guys on the larger side will likely not experience this as much or at all.
Is bottom growth avoidable? People say it's ugly :(
Like (potential) male pattern baldness and vocal chord lengthening, clitoral growth is not avoidable. The amount of growth is variable person to person. On average, a "fully grown" erect testosterone-ified clitoris will be 1 to 3 inches. Some people on the intersex spectrum may experience larger growth.
Do I need to care for my bottom growth?
Yes! Similarly to a natal penis*, a T-penis will grow foreskin, which requires regular cleaning. A little soap and water in the shower works just fine.
*natal penis= the penis someone assigned-male-at-birth has
Will testosterone fix all my problems?
As nice as that would be, no. Taking testosterone HRT will certainly boost your self confidence by making your body align more closely with your perceived self, but any personal self-growth has to come from you. Testosterone is merely a tool to help you achieve peace.
Bibliography
Coleman, E., A. E. Radix, W. P. Bouman, G. R. Brown, A. L. de Vries, M. B. Deutsch, R. Ettner, et al. “Standards of Care for the Health of Transgender and Gender Diverse People, Version 8.” International Journal of Transgender Health 23, no. sup1 (August 19, 2022). https://doi.org/10.1080/26895269.2022.2100644.
“Hormones - Masculinising.” TransHub, October 27, 2025. https://www.transhub.org.au/medical/hormones-masculinising/.
Kirkley, Jerrica. “What You Need to Know About Testosterone-Based (Masculinizing) Hormone Therapy.” Edited by Christina Aungst. GoodRX, August 30, 2023. https://www.goodrx.com/health-topic/lgbtq/testosterone-gender-affirming-hormone-therapy-transgender-care.
Memorial Sloan Kettering Cancer Center. “How to Give Yourself a Subcutaneous Injection Using a Prefilled Syringe.” Memorial Sloan Kettering Cancer Center, December 7, 2023. https://www.mskcc.org/cancer-care/patient-education/how-give-yourself-subcutaneous-injection-using-prefilled-syringe.
Rostom, Mary, Ranjith Ramasamy, and Taylor P. Kohn. “History of Testosterone Therapy through the Ages.” International journal of impotence research, November 2023. https://pubmed.ncbi.nlm.nih.gov/35075296/.
Salvo, Victor. “Dr. Michael Dillon - Nominee.” Legacy Project Chicago. Accessed September 4, 2025. https://legacyprojectchicago.org/person/michael-dillon.
“Testosterone: For Transmen, Transmasculine, Non-Binary and Gender Expansive Folks.” Gender Confirmation Center, April 8, 2025. https://www.genderconfirmation.com/blog/testosterone-for-transmen-transmasculine-non-binary-gender-affirming/.
“Testosterone Gel for Gender-Affirming Hormone Therapy: What, Where, and How.” FOLX Health. Accessed May 10, 2026. https://www.folxhealth.com/library/testosterone-gel-hrt-what-where-how.
Vance, Dwight A. “Premarin: The Intriguing History of a Controverisal Drug.” International journal of pharmaceutical compounding, July 2007. https://pubmed.ncbi.nlm.nih.gov/23974785/.
Plus personal accounts from other trans guys.

Comments